
There are an estimated 1.4 billion overweight people in the world, of whom 500 million are obese. Typical of the actions performed by the World Health Organization (WHO) is a visit to Tashkent, Uzbekistan, for a three-day workshop, described by the WHO website:
Twenty participants from the fields of health, public education, community, sports and physical activity, food production, research and science worked with WHO experts in setting priority actions and identifying the roles and responsibilities of the different sectors.
The country’s Ministry of Health and the WHO team identified the area’s chief problems as high-fat and high-sugar foods (including soft drinks, of course) and kids spending too much time with electronic devices. This gathering even included a representative from neighboring Kazakhstan.
WHO had codified the recommended tools for childhood obesity management at the national level, in a guidebook, called “Prioritizing areas for action in the field of population-based prevention of childhood obesity,” which can be downloaded in English or French.
Further details about the guidebook include:
Three priority-setting approaches are described in this document: the WHO Stepwise framework for preventing chronic disease, the Modified Problem/Solution Tree (mPAST) process and the ANGELO (Analysis Grid for Elements Linked to Obesity) process. All three approaches follow four common steps which include:
- Problem identification and needs analysis
- Identification of potential solutions
- Assessment and prioritization of potential solutions
- Strategy development
Last month, NBC News came out with a shocking headline: “New Zealand’s solution for rising health costs? Deport fat people.” Art Caplan told the story of an obese professional chef named Albert Buitenhuis who had moved to New Zealand six years previously with his wife. Although both still South African citizens, they were technically, like all permanent residents of New Zealand, entitled to free medical care funded by taxes.
New Zealand is the third most obese “developed world” country, after the U.S. and Mexico. Caplan points out that the country does not deport people for being smokers, or for having sexually transmitted diseases, both of which are a drain on the health care system and besides, pose something of a threat to other people. But this didn’t matter when it came to the Buitenhuis couple. Caplan wrote:
They are now facing deportation after their work visas were declined because of his weight. New Zealand immigration authorities cited the demands his obesity could place on New Zealand’s health services in terms of cost.
Their case is currently under appeal to the Minister of Immigration.
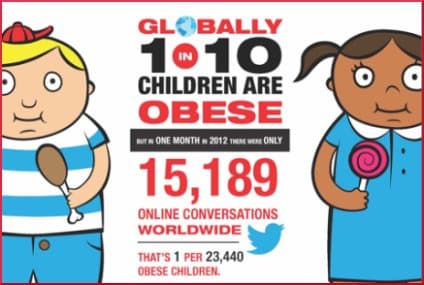
GLOBALHealthPR is a network of independent public relations agencies concerned with healthcare in 17 different countries, and their contention is that childhood obesity is a global problem that lacks an appropriate global conversation. The U.S. Director of Digital Strategy, Anthony LaFauce, says:
While levels of childhood obesity are rising worldwide, the levels of conversation around this disease are not sufficient to effect change. Healthcare providers, policymakers, industry and advocacy groups have the opportunity and the obligation to use social media to increase targeted education and awareness around childhood obesity.
The picture on this page is part of their infographic, but it wouldn’t all fit, so please go to their website and see the whole thing.
Your responses and feedback are welcome!
Source: “Uzbekistan identifies priority actions for tackling childhood obesity,” Euro.WHO.int, 11/16/12
Source: “New Zealand’s solution for rising health costs? Deport fat people,” NBCNews.com, 08/11/13
Source: “Global Healthcare Communications — a better way,” GLOBALHealthPR
Image by GLOBALHealthPR.
 FAQs and Media Requests:
FAQs and Media Requests: 











